- Ben Haresign
- 01 Jun, 2026
- Data & Analytics
- 6 min read
NWRS Is Not Just a Return: Using Workforce Trends to Support GP Reimbursement Evidence
NWRS Is Not Just a Return
Using workforce trend data to support GP reimbursement evidence, understand capacity movement and build a clearer practice workforce story.
What the tool helps show
- ✅ GP WTE movement
- ✅ Clinical workforce change
- ✅ Patients per WTE pressure
- ✅ Peer benchmarking
- ✅ Reimbursement evidence notes
NWRS is often treated as a monthly workforce return. Someone updates the figures, submits the data, and the practice moves on.
But with the introduction of the practice-level GP reimbursement scheme in 2026/27, NWRS has become more than an administrative task. Used properly, it can help practices understand workforce movement, capacity change, patient pressure and the evidence trail behind GP reimbursement claims.
It does not replace payroll, contracts, rotas or local employment records. But it can help tell the workforce story. And that story now matters.
Core message
NWRS shows the trend. Local records prove the reason. Together, they help create a stronger evidence trail.
Important: NWRS does not prove a claim on its own
NWRS can support an evidence trail, but practices still need local records such as payroll, contracts, rota records, session changes, approval notes, funding records and claim submissions.
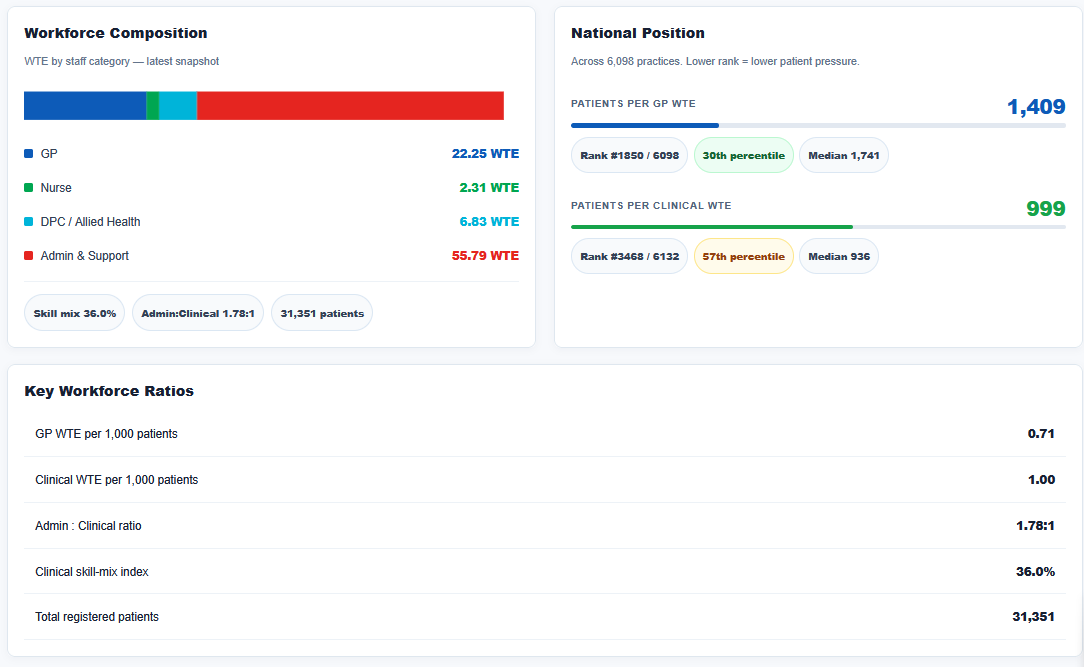
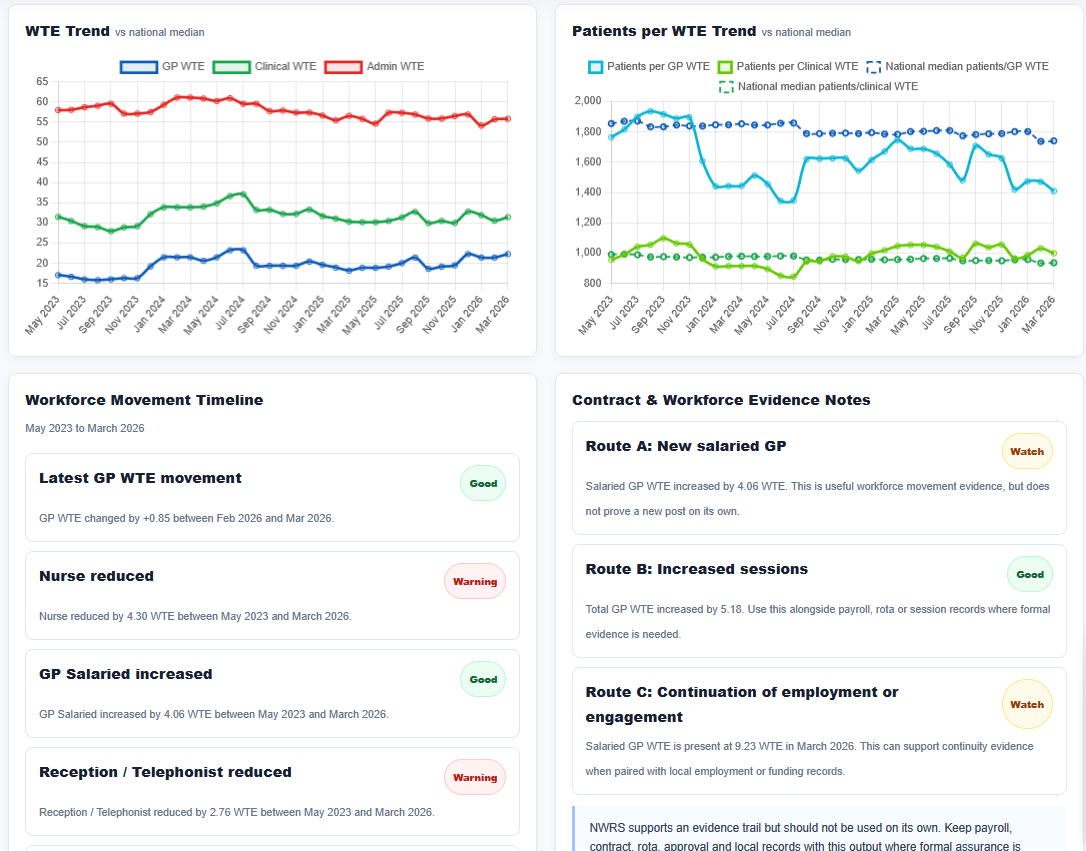
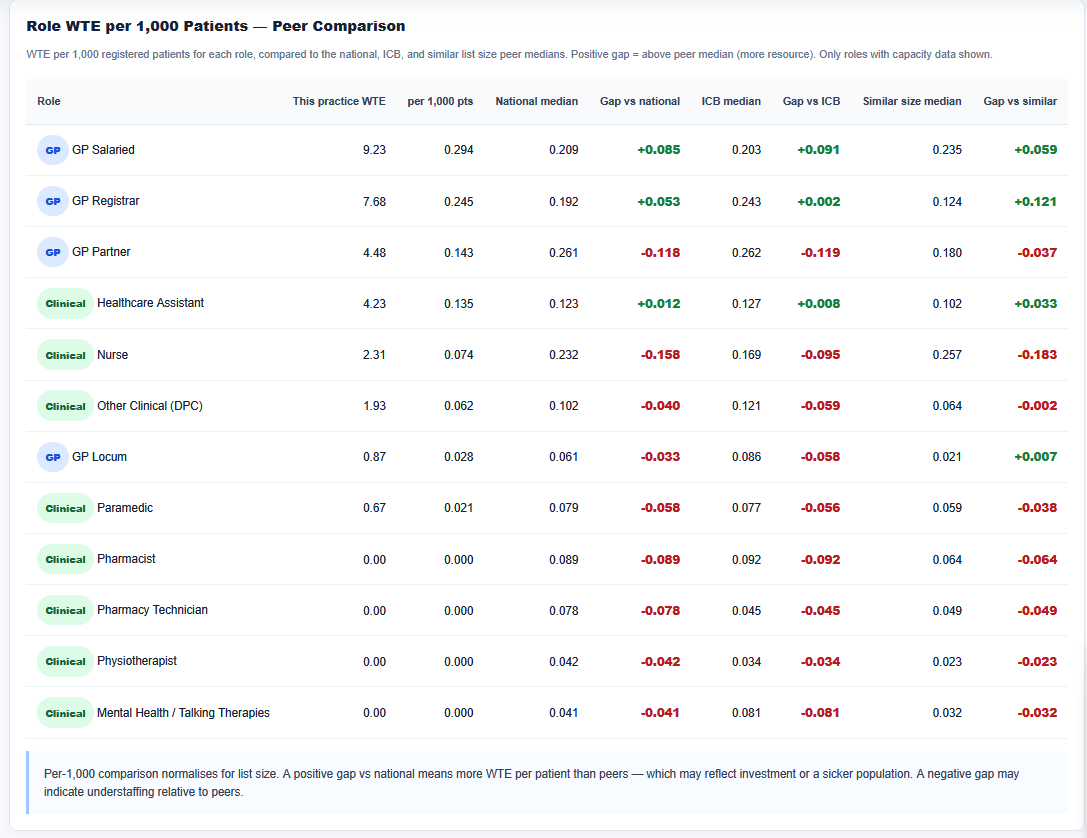
Example output from the NWRS Workforce Evidence Tool, showing WTE trends, patient-per-WTE pressure, movement timelines and benchmarking.
Why NWRS matters more in 2026/27
The 2026/27 GP contract introduces a practice-level GP reimbursement scheme. NHS England has confirmed that funding is being repurposed from the former PCN-level Capacity and Access Payment to support practices to recruit new GPs or increase GP sessions from existing GPs.
That creates a practical issue for practices. It is not enough to say:
“We increased GP capacity.”
Practices need to be able to show what changed, when it changed, and how that movement is supported by local evidence.
That is where NWRS can become useful. It gives practices a structured way to look at workforce trend data over time, especially when comparing a baseline point with a later workforce snapshot.
NWRS supports the evidence trail
Route A: New salaried GP
Salaried GP WTE movement may support the evidence trail, but it does not prove a new post on its own.
Route B: Increased sessions
Total GP WTE movement can help evidence additional capacity when paired with payroll, rota or session records.
Route C: Continuation
Continued salaried GP WTE can support continuity evidence when paired with employment or funding records.
What a workforce trend can show
A single NWRS snapshot is useful. A trend is better.
Looking across multiple months allows a practice to identify whether workforce change is sustained, temporary, recent or part of a longer-term shift.
For example, a practice may want to understand whether GP WTE has increased, whether salaried GP WTE has changed, whether registrar movement is distorting the picture, or whether patients per GP WTE has improved.
Useful questions to ask from NWRS trend data
- Has GP WTE increased since the baseline?
- Has salaried GP WTE changed?
- Has GP registrar WTE distorted the overall GP position?
- Has clinical WTE increased because of GP growth, nursing growth or DPC roles?
- Has admin WTE reduced while clinical WTE increased?
- Have patients per GP WTE improved?
- Are changes visible over 3 months, 6 months and 12 months?
- Does the trend match what the practice believes happened locally?
Patients per WTE gives the workforce story context
Workforce planning is not just about headcount. It is about pressure.
A practice with rising GP WTE may still be under significant strain if list size has grown faster than the workforce. Equally, a practice may have fewer GPs than another practice but a lower patients-per-GP-WTE ratio.
Patients per GP WTE
Helps show direct GP capacity pressure and whether additional GP workforce is improving the practical position.
Patients per clinical WTE
Gives a broader view of clinical capacity, including nursing and direct patient care roles.
Benchmarking helps avoid assumption-led planning
Practice workforce data is easy to misread in isolation. A GP WTE figure may look high or low, but without context it does not tell the full story.
Benchmarking helps practices understand whether their workforce pressure is above or below peer groups.
- National median
- Same ICB
- Same sub-ICB
- Same NHS region
- Similar list-size practices
Role movement matters
Not all workforce movement means the same thing.
A rise in total GP WTE could come from a new salaried GP, increased sessions from an existing GP, a GP registrar, a locum arrangement, a coding change or correction of previously inaccurate NWRS data.
These all tell different stories. For reimbursement evidence, the distinction matters.
Practical check
If the data shows a movement the practice does not recognise, check the NWRS coding before relying on it for planning, benchmarking or reimbursement evidence.
The evidence trail should be built now
The biggest risk is waiting until the claims process is open before building the evidence trail. By then, practices may be trying to reconstruct workforce history from old rotas, payroll exports, emails, appointment books and half-remembered conversations.
Identify the role, person or workforce group.
New post, extra sessions, continuation or role movement.
Match the movement to payroll, rota and NWRS dates.
Keep contracts, approvals, session records and funding notes.
How the NWRS Workforce Evidence Tool helps
I have built a new NWRS Workforce Evidence Tool to help practices review workforce movement between two reporting snapshots.
The aim is not to replace local judgement. The aim is to make the workforce trend visible enough that practices can ask better questions.
The tool reviews:
- GP WTE movement
- Clinical WTE movement
- Admin and support WTE movement
- Role-by-role changes
- 3, 6 and 12 month trends
- National and local benchmarks
- Reimbursement evidence notes
The key message
NWRS is not just a return. It is workforce intelligence.
For the GP reimbursement scheme, it can help support the evidence trail, but it should always be paired with local records.
For workforce planning, it can show whether capacity is improving, pressure is reducing, and whether the practice is moving in the right direction.
The real value is not the number on its own. The real value is the story behind the number.
NWRS shows the trend. Local records prove the reason.
Check your NWRS workforce trend now
Do not wait until the claim window opens to start building the evidence trail from old rotas, payroll exports and mystery spreadsheets.
This article is intended to support practical workforce planning and evidence preparation. Practices should pair NWRS outputs with their own local employment, payroll, rota and funding records.